Glioblastoma kills most patients within 18 months. Between quarterly MRI scans, tumors grow unchecked — silent, aggressive, indifferent to the calendar. A San Francisco startup placed a wireless brain implant in three people during tumor surgery at Royal Melbourne Hospital, according to Wired, aiming to watch cancer’s electrical activity in real time and eventually disrupt it with targeted stimulation. The implants stayed in for about 30 minutes — a safety check, not a cure. The ambition behind them, however, is enormous.
Cancer as a Network Problem
Coherence Neuro is reframing brain tumors as electrical malfunctions — and building the device to match.
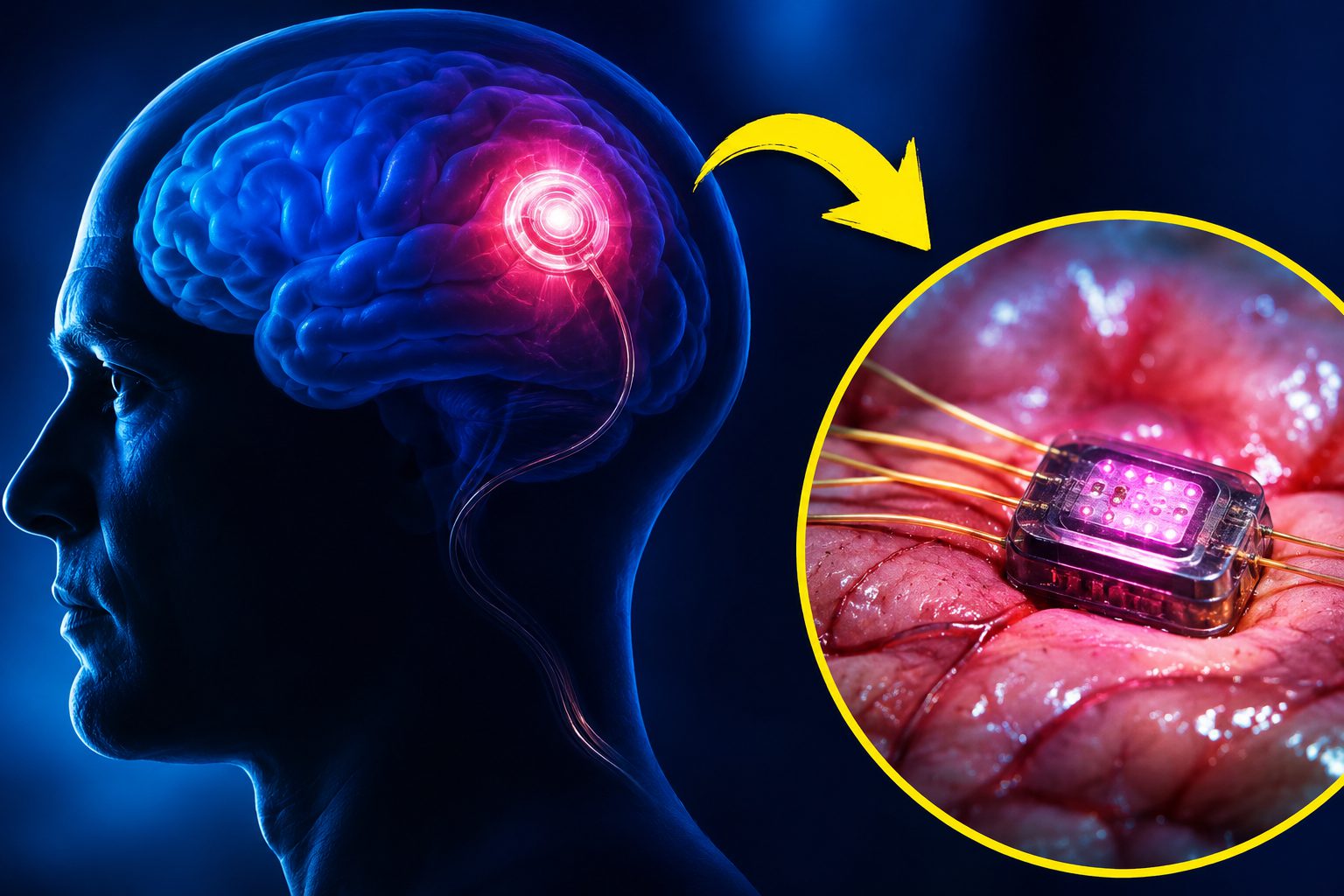
Coherence Neuro CEO Ben Woodington frames brain tumors the way most people think about epilepsy. “These are electrical conditions, just like epilepsy, just like depression. This is a network problem in the brain,” he told Wired. The science backs the framing, at least partially. Stanford researchers showed in 2019 that high-grade gliomas form actual synapses with neurons, hijacking the brain’s wiring like a parasite plugging into the grid. Coherence’s SOMA implant — coin-sized, wireless, threaded with ultra-thin microwires — is designed to read a tumor’s electrical fingerprint, decode it with AI, and deliver targeted stimulation to disrupt it. Continuously. Around the clock.
The trial at Royal Melbourne Hospital represents the first time a BCI has been tested explicitly to detect and suppress cancer rather than restore movement or communication. Three patients received temporary intraoperative implants; long-term implantation is the next phase, pending safety data. SOMA pairs:
- a skull-embedded implant
- an over-ear wearable for power
- a clinician-facing app for real-time oversight
The device is MRI-transparent, designed to coexist with standard imaging follow-up. Neuralink’s head neurosurgeon Matthew MacDougall serves as an advisor and investor — a detail that earns its own sentence. Coherence has raised roughly $10 million in seed funding, according to medtech industry reports; FDA clearance remains years away.
Not the First Electric Cancer Play
SOMA’s closest predecessor is already on the market — and already showing the limits of external delivery.
Novocure’s Optune delivers tumor-treating fields through adhesive scalp patches and extends glioblastoma survival by months, but requires a shaved head, visible arrays, and a battery backpack. SOMA aims to bury the therapy directly at the tumor site, inside the skull, with none of the conspicuous hardware. Professor Kate Drummond at Royal Melbourne Hospital described the trial as offering “unprecedented insights” into brain tissue treatment evaluation, according to the hospital’s announcement. The current implants were temporary; permanent implantation awaits the next trial phase.
The Honest Risks Nobody Wants to Headline
The science is promising, but the obstacles — biological, technical, and ethical — are substantial.
Skepticism here is not cynicism — it is math. Glioblastoma is biologically heterogeneous; one bioelectric approach will not necessarily work across patients, and the therapy mechanism remains unproven at scale. Invasive implants carry:
- infection
- bleeding
- hardware failure risks
Independent neuro-oncologists have also flagged a challenge that rarely makes headlines: continuous neural recordings from a brain implant represent extraordinarily sensitive personal data, transmitted wirelessly, managed by a startup still operating on seed funding. Robust cybersecurity and clear data-governance frameworks are not optional extras — they are prerequisites.
What Comes Next
The outcome of these early trials will determine whether bioelectric oncology becomes a new category or an expensive footnote.
If SOMA demonstrates benefit, oncology may begin treating certain cancers less like static masses and more like cardiac arrhythmias — manageable, modulatable, monitored in perpetuity. A cancer vaccine analogy applies here too: if the evidence does not follow, this becomes a cautionary chapter in the long history of promising implantables that stalled between first-in-human and pivotal trial. Three patients in Melbourne sit at that crossroads. The outcome remains unknown.