America’s 10,000+ transplant patients face a brutal waiting game, but MIT’s injectable solution could flip that math. Professor Sangeeta Bhatia’s team figured out how to pack liver cells into hydrogel microspheres that flow like liquid through a syringe, then solidify into functional “satellite livers” wherever doctors inject them.
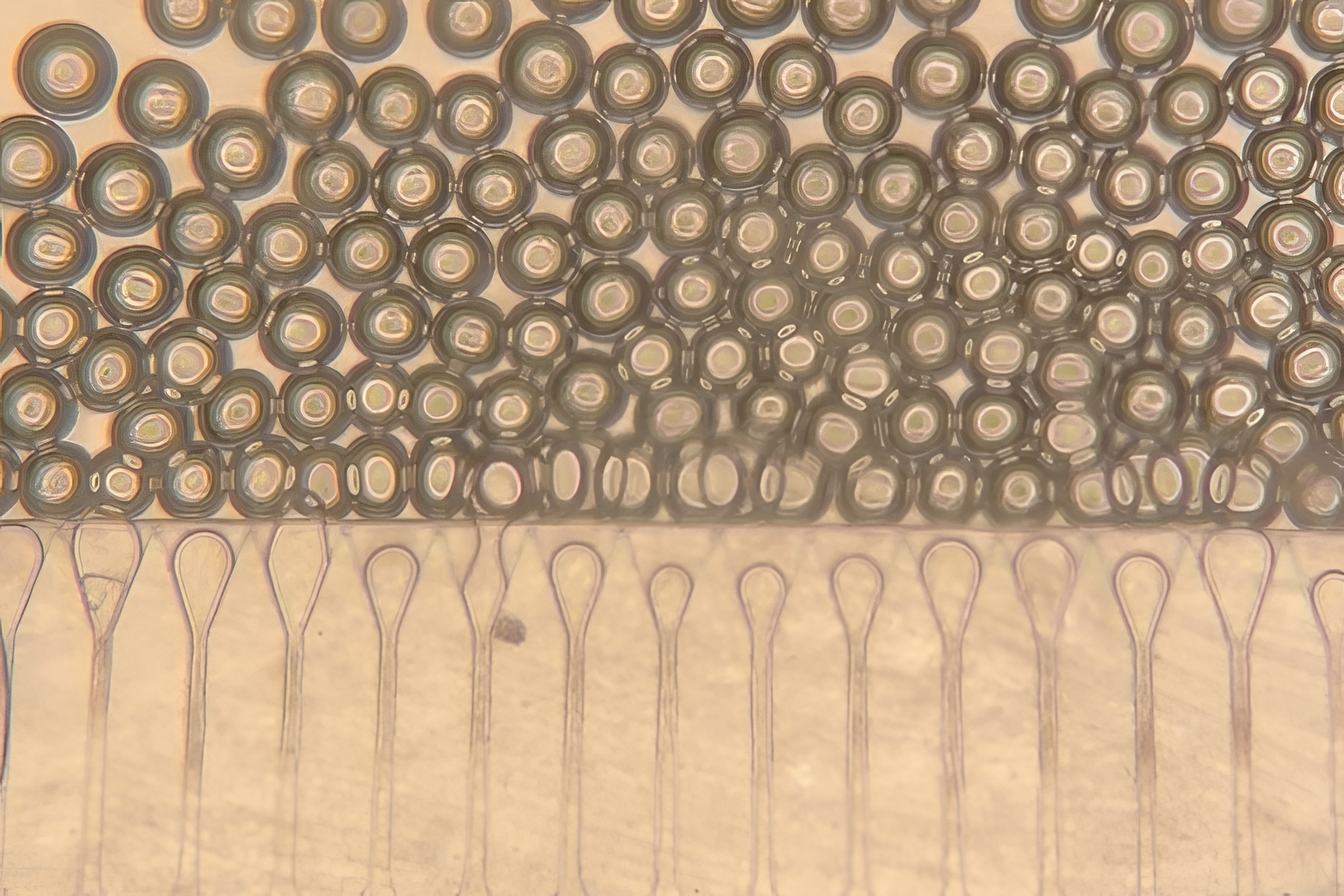
Think of it like biological IKEA furniture—flat-packed cells that assemble themselves once delivered. The INSITE technology (Injected, Self-assembled, Image-guided Tissue Ensembles) mixes hepatocytes with tiny gel spheres and supportive fibroblasts, creating grafts that actually work for eight weeks in mouse studies.
The microspheres act like cellular Airbnbs, giving liver cells a safe place to thrive while blood vessels move in.
“These microspheres provide the hepatocytes with a niche where they can stay localized and become connected to the host circulation much faster,” according to researcher Vardhman Kumar. The genius lies in the delivery system—doctors use ultrasound guidance to inject these tissue cocktails into abdominal fat, nowhere near the failing liver.
Your body doesn’t seem to mind the geographic confusion. The injected grafts produced proper liver enzymes and proteins while integrating with existing blood vessels, vastly outperforming naked cell injections that typically die within days. After eight weeks, these satellite livers remained viable and functional—a biological moonshot that actually landed.
MIT’s approach faces competition from LyGenesis, which grows mini-livers inside lymph nodes and has already started human trials. Their mouse studies showed 30-week survival, but require more invasive procedures. Other research focuses on organoids for drug testing rather than actual therapy, making Bhatia’s work particularly significant for real-world treatment.
The MIT team calls these “injectable, self-assembling niches,” representing “a significant step toward regenerative treatments.” Translation: we might actually solve organ shortages without waiting for lab-grown replacements or xenotransplantation breakthroughs.
Current limitations include requiring immunosuppressive drugs, but future iterations could use “stealth” cells or local drug delivery to avoid that complication. For the thousands facing liver failure who can’t undergo surgery, injectable tissue engineering offers hope that fits in a syringe.
Human trials remain years away, but Bhatia’s decade of microliver research suggests this isn’t just another lab curiosity destined for academic obscurity.